18Y MALE WITH ONE EPISODE OF SEIZURES
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome.
CASE:
18Y male came with complaints of involuntary movements of both upper and lower limbs
CHIEF COMPLAINTS:
Involuntary movements of both upper and lower limbs
HISTORY OF PRESENT ILLNESS:
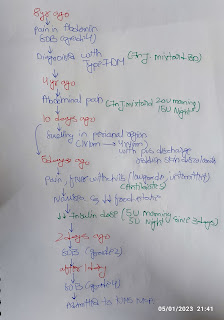
Patient was apparently asymptomatic 1 day ago , then he developed involuntary movements ,in both upper and lower limbs, which was sudden in onset , associated with shivering,and fever.
He complained of nausea and pain after dinner in the epigastrium which was radiating towards right Iliac fossa and was pricking type with no aggregating factors and relieved on taking medication
There was also history of Shortness of breath 1 hr after playing.
At 11.30 pm he was studying, then was feeling uneasy after which he developed involuntary movements of both limbs.
no history of post-ictal confusion,uprolling of eyeball,tongue bite, involuntary defecation and micturation.
PAST HISTORY:
•No history of HYPERTENSION,DIABETES MELLITUS ,ASTHMA, EPILEPSY, TUBERCULOSIS.
PERSONAL HISTORY:
•DIET:MIXED
•APPETITE:NORMAL
•SLEEP: ADEQUATE (8hrs of sleep)
•BOWEL AND BLADDER MOVEMENTS:REGULAR
•ADDICTIONS:NO
•ALLERGY:NO
FAMILY HISTORY:
•Not significant
GENERAL EXAMINATION:
•Patient was conscious,coherent and cooperative,well oriented to time place and person,moderately built and moderately nourished.
•Pallor:- absent
•Icterus:- absent
•Cyanosis:- absent
•Clubbing:- absent
•Lymph nodes:- absent
•Edema:- absent
VITAL SIGNS:
•TEMPERATURE: Afebrile
•BP:140/80 mm Hg
•RR: 22/min
•Spo2:99
•GRBS:130 mg%
SYSTEMIC EXAMINATION:
CVS:S1,S2 heard,no murmurs
RESPIRATORY SYSTEM:
trachea central in position
Normal vesicular breath sounds heard
BAE ++
CNS EXAMINATION:
The patient is well oriented to time, place,person.
CRANIAL NERVES EXAMINATION:
All the cranial nerves are intact and functioning.
MOTOR EXAMINATION:
Power
Rt UL-5/5. Lt UL-5/5
Rt LL-5/5. Lt LL-5/5
Tone-
Rt UL -N
Lt UL-N
Rt LL-N
Lt LL-N
Reflexes:. RIGHT LEFT
Biceps. ++ ++
Triceps ++ ++
Supinator. ++ ++
Knee. ++ ++
Ankle. ++ ++
Plantar:. Flexion Flexion
•SENSORY EXAMINATION
crude touch N N
Pain N N
Temperature N N
Fine touch N N
Vibration Right Left
Upper limb. 15 sec 15 sec
Lower limb. 11 sec. 10sec
Tibia. 14 sec. 14sec
Toe. 15sec. 15sec
Finger nose co-ordination : +
ABDOMEN EXAMINATION:
Inspection :- no scars
Palpation :- soft,non tender
Auscultation :- BOWEL SOUNDS



Investigations....







PROVISIONAL DIAGNOSIS:
SEIZURES
MANAGEMENT:
symptomatic management is administered

Comments
Post a Comment