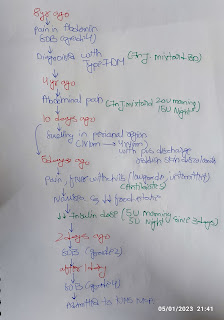
58 yr old female with complaints of shortness of breath
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
I have been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
A 58 year old female resident of munugodu , daily wage labour by occupation Brought to causuality with cheif complaints of shortness of breath since 3 days.



SYSTEMIC EXAMINATION:
Respiratory system:
Patient is examined in sitting postion
Inspection:
Upper respiratory tract- oral cavity, nose , oropharynx appears normal
Chest appears BILATERALY symmetrical and elliptical in shape
Respiratory movements appears equal on both sides and it is abdominothoracic type
Trachea is central in position and nipples in fourth intercostal space
No dilated veins ,scars,visible pulsations
Palpation: All Inspectory findings are confirmed on Palpation
Trachea is central in postion.
Respiratory movements : normal on both sides
Tactile vocal fremitus : increases in INFRAAXILLARY and infrascapular area.

BASAL Crepitations were heard on the day of admission.
CVS EXAM
S1 S2 heard ++
No murmurs are heard. Apex beat at 6th intercostal space
Cns examination.....
no focal neurological deficits
Cranial nerves are intact
ABDOMINAL EXAMINATION:
INSPECTION
No distension
- Umbilicus - normal in position
- Equal symmetrical movements in all the quadrants with respiration.
- No visible pulsation ,peristalsis, dilated veins and localized swellings.
- No scars, sinuses, hernial orifices are seen
PALPATION
- SUPERFICIAL : There is no local rise of temperature
- DEEP: no organomegaly
PERCUSSION: tympanic note heard
AUSCULTATION: bowel sounds heard
INVESTIGATIONS:
Chest x ray :
Increased C:T ratio — cardiomegaly
Obscuration of costophrenic angle.

2/11/2022.....


3/12/2022....










Usg findings..
Bilateral pleural effusion with underlying
Lung collapse.






Provisional diagnosis :
PROVISIONAL DIAGNOSIS
- Chronic heart failure with Cardiomegaly and Bilateral pleural effusion
- Chronic kidney disease
- severe anemia
TREATMENT:
1. INJ LASIX 40mg IV TID
2.T.NODOSIS 250 mg PO TID
3. T.NICARDIA 10mg PO TID
4.T SHELCAL 500mg PO OD
5.CAP BIOD3 PO OD
6.INJ ERYTHROPOIETIN 4000IU,WEEKLY ONCE IV.
7.INJ OROFERS 100mg IN 100ml,NS IV WEEKLY ONCE.


Comments
Post a Comment