This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan..
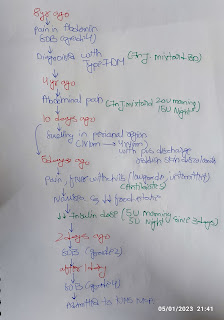
57yr old male came to casualty complaining of shortness of breath since 10days, bilateral pedal edema since 6days, generalized itching since 6days,
He was alright until 6 months ago when he noticed a small wound in his left leg.
It was itchy around the site and he began to scratch the site constantly until it bleed a month later.
He complained of swelling and pain in his left leg due to which he was taken to local hospital. where he was diagnosed to have Thrombus in distal popliteal artery of left side and at the same time he was told that he had Hypertension and type 2 diabetes mellitus.
He underwent Left Popliteal artery thrombectomy when he was diagnoised with thrombus 6 months ago.
He took epospirin and vit k antagonist for 15 days.
He has been irregular with oral antiglycemics and has not taken any medication for hypertension since then.
he was told to have Bronchial asthma 3yrs ago following an episode of difficulty in breathing and used rotahaler.
he is currently complaints of shortness of breath since 10days, bilateral pedal edema since 6days, generalized itching since 6days.
personal history-
Has normal diet and appetite.
Reduced urination frequency and regular bowel habits .
Sleep- adequate
Appetite is normal.
No history of use of any substance.
on examination-
General examination
pt was Conscious coherent cooperative well orientated to time place person.
Afebrile
BP- 150/100
PR- 90
RR- 20
SPO2- 94 % at RA
Systemic examination
CVS S1 S2+
RS- BAE+, NVBS
PA- Soft, non tender
CNS- no FND .
ABNORMAL PARAMETERS. .
Renal function tests
Urea 128mg/dl
Creatinine 8 mg/dl
Uric acid 7.3mg/dl
Phosphorus 7.9mg/dl
Blood urea - 123mg/dl
ABG
Ph 7.24
Pco2 23.8 mgHg
Po2 49.7mgHg
CUE
Albumin +++
Sugar - trace.
HEMOGRAM
Hb 10.7 mg/dl
Lymphocytes 18%
Eosinophils 26%
PCV 32.5 vol%
RDW-cv 14.3%
Fever chart
ECG
Provisional diagnosis
- chronic kidney disease with diabetic nephropathy with metabolic acidosis .
-pityriasis versicolor.
-hypertension and diabetes Mellitus.
Plan of management..
Salt restrictions less than 2.4 g per day
fluid restriction less than 1 litre
per day tablet lasix 40 mg p.o t.i.d
tab orofer XT PO OD
tab shelcal 500 mg PO OD
tab nicardia 10 mg PO OD
tablet nodosis 55
injection erythropoietin 4000 IU s/c weekly once
injection iron sucrose 1 ampule in hundred ml NS during dialysis.
MEDICATIONS ..
Soap notes .
subjective patient has more fresh complaints
objective
patient is C/C/C
blood pressure 150/ 90
PR 100 BPM
CVS S1 S2 present
RS BAE present
assessment CKD diabetic nephropathy stage 5 with metabolic acidosis known case of diabetes mellitus since 2 months
Rx plan. .
fluid restriction less than 1 litre per day salt restriction less than 2.4 g per day
tab lasix 40 mg PO bid
tab nodosis 500 mg PO bid
tab orofer XT pure OD
tab shelcal CT 500 mg OD
tab nicardia 10 mg BD
injection piptaz 4.5 g IV BD
injection albumin 20% lv
tab levocetirizine OD HS
injection erythropoietin 4000 IU sc..
Soap notes
AMC cubicle
SUBJECTIVE
patient has no fresh complaints
OBJECTIVE
patient is C/C/C
blood pressure 150/ 90
PR 100 BPM
CVS S1 S2 present
RS BAE present
ASSESSMENT CKD diabetic nephropathy stage 5 with metabolic acidosis known case of diabetes mellitus since 2 months
PLAN
fluid restriction less than 1 litre per day salt restriction less than 2.4 g per day
tab lasix 40 mg PO bid
tab nodosis 500 mg PO bid
tab orofer XT pure OD
tab shelcal CT 500 mg OD
tab nicardia 10 mg BD
injection piptaz 4.5 g IV BD
injection albumin 20% lv
tab levocetirizine OD HS
injection erythropoietin 4000 IU sc
calamite lotion
candid cream LA
liquid paraffin .
Impressions of USG doppler on aug 13
THROMBOTIC OCCLUSION OF CFA AND PROXIMAL SFA CAUSING HEMODYNAMICALLY SIGNIFICANT CHANGES IN DISTAL BRANCHES > MONOPHASIC WAVE FORM IN EIA-TO R/O PROXIMAL OCCLUSION