17 year old girl with diabetic ketoacidosis
17 YEAR OLD GIRL WITH DIABETIC KETOACIDOSIS
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
A 17 year old girl , studying 10th class, hailing from Janapahad near Miryalaguda , presented to the OPD with chief complaints of fever and vomitings since yesterday ( 05/11/22 ) morning .
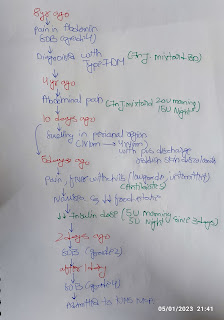
History of presenting illness : The patient was apparently asymptomatic 7 years back . In 2015 , she got fever with 4-5 episodes of vomitings for which was taken to Nilofer where she was admitted for 1 month , they performed blood sugar tests and she was then diagnosed with type - 1 diabetes mellitus .
In 2018 , she again had 2 episodes of vomitings with very high sugar levels when checked with the glucometer , she was admitted in KIMS Narketpally for 5 days .
Now again in 2022 , she had missed her morning dose of insulin and morning breakfast yesterday ( 05/11/22 ) as she woke up late . She presented to the OPD with fever and had 8 episodes of vomitings which were non bilious , non projectile with food as contents . She also complained of SOB for a very brief period on lying down , she was taken to a local doctor where when checked the blood sugars were 550 mg/dl for which insulin dose was given . She was then referred to KIMS Narketpally .
She also complains of excessive thirst when she has high sugar levels .
Past history : The patient was diagnosed with type 1 diabetes mellitus 7 years back .
She is not a K/C/O HTN , asthma , TB , thyroid disorders , epilepsy.
Personal history : The patient wakes up between 7-7:30 am in the morning, takes her insulin dose, has her breakfast. She goes to school at 9 am by walking, has her lunch at school itself and returns home at 5 pm . She does her homework and studies till 9 pm, then takes her insulin dose, eats dinner and sleeps by 9:30 pm .
Diet - mixed ( consumes chicken weekly once )
Appetite - normal
Sleep - adequate ( from 9:30 pm to 7:30 am )
Bowel and bladder movements - regular
Family history :
The patient's paternal grandfather ( expired ) is diabetic . The maternal grandfather is diabetic since 8 years and maternal grandmother is diabetic since 4 years , both of them are on oral hypoglycemic drugs since then .
The patient is on insulin therapy since 7 years .
She takes 10 units of insulin ( 5 units of IPH insulin and 5 units of HAI ) twice daily , once before breakfast and once before dinner .
For the first 6 months of therapy , she has been injecting around the umbilicus , later on she has been injecting into her deltoid muscle .
Everyday she checks her blood sugar levels with glucometer in the morning and evening .
She has been having spikes in her sugar levels all along .
General Examination : The patient is conscious, coherent and cooperative, well built and nourished .
Pallor, icterus, cyanosis, clubbing, pedal edema and generalised lymphadenopathy are absent .

VITALS :
06/11/22 :
Temperature - afebrile
BP - 110/70 mm Hg
HR - 90bpm
RR - 18 cpm
07/11/22 :
Temperature - afebrile
BP - 110/70 mm Hg
HR - 80 bpm
RR - 18 cpm
08/11/22 :
Temperature - afebrile
BP - 100/70 mmHg
HR - 100 bpm
RR - 18 cpm
Systemic Examination :
CVS :
On palpation ‐
• Apex beat was felt in the left 5th intercostal space medial to the mid clavicular line.
• JVP was normal
• No precordial bulge
• No parasternal heave
On auscultation ‐ S1, S2 heard , no murmurs
RS :
On inspection ‐
• Chest is bilaterally symmetrical
• Expansion of chest: Equal on both sides
• Position of trachea: Central
• No visible scars, sinuses, pulsations
On palpation :
• Expansion of chest was equal on both sides.
• Position of trachea: Central
• Tactile Vocal Fremitus: resonant note was felt.
On percussion: all lung areas were resonant
On auscultation :
• Bilateral air entry was present, normal vesicular breath sounds were heard.
• Vocal resonance: resonant in all areas
P/A : soft, non tender, no organomegaly, no distension, bowel sounds heard.
CNS : The patient is well oriented to time, place, person.
Higher mental functions are intact.
Cranial nerve examination :‐
All cranial nerves are intact and functioning.
Motor System Examination :‐
• Normal bulk in upper and lower limbs
• Normal tone in upper and lower limbs
• Normal power in upper and lower limbs
• Gait is normal
. Reflexes are normal .
Sensory System Examination :‐
Normal sensations are felt in all the dermatomes.
No cerebellar signs .
No meningeal signs.
Investigations :















Provisional Diagnosis : Diabetic Ketoacidosis
Treatment :
06/11/22 :
1) Inj. Human Actrapid Insulin infusion 4 ml/hr for 5 hrs , then 2 ml/hr for the next 5 hrs .
2) IV fluids - NS /RL /5% dextrose at 100 ml/hr
3) Inj. Pantop 40 mg IV OD
4) Inj. Zofer 4 mg IV BD
5) Inj. Monocef 1 gm IV BD
6) Inj. Piptaz 4.5 gm IV TID
7) Inj. Neomol 1 gm IV SOS ( if temperature > 101 F )
07/11/22 :
1) Inj. Human Actrapid Insulin infusion 4 ml/hr for 5 hrs , then 2 ml/hr for the next 5 hrs .
2) IV fluids - NS /RL /5% dextrose at 100 ml/hr
3) Inj. Pantop 40 mg IV OD
4) Inj. Zofer 4 mg IV BD
5) Inj. Monocef 1 gm IV BD
6) Inj. Piptaz 4.5 gm IV TID
7) Inj. Neomol 1 gm IV SOS ( if temperature > 101 F )

Comments
Post a Comment