45 year old male with Abdominal distension and pedal edema.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment .
CASE:-
45 year old male complaints of abdominal distension and b/l pedal edema (pitting type) , shortness of breath and scrotal swelling.
CHIEF COMPLAINTS:-
Patient complaints of
•Abdominal distension
•B/l pedal edema
•Shortness of breath
•scrotal swelling
Since 25 days
HISTORY OF PRESENTING ILLNESS:-
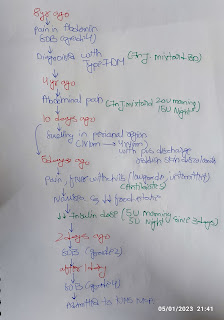
Patient was apparently asymptomatic 6 years ago, then he had swellings over chest for which he went to hospital and was diagnosed as diabetic and was on medication since then.
•2 years ago when he went for routine checkup he was diagnosed as hypertensive and was on medication .
•6 months back patient's speech was reduced for which he went to a local hospital where he was found to have low GRBS (27 mg/d) and he
also had jaundice and was advised to stop consuming alcohol.
•25days back he developed scrotal swelling, pedal edema, abdominal distension which was insidious in onset and gradually progressive, he also exhibited shortness of breath, for which he went to an RMP and was referred to KIMS, Narketpally.
PAST HISTORY:-
*H/O DM since 6 years and used tab.glibenclamide 5mg+ metformin 500mg, stopped taking medication since 6 months *H/O HTN since 2 years and taken Tab. Telma 40mg.
FAMILY HISTORY:- Insignificant.
PERSONAL HISTORY:-
•Diet:- mixed
•Appetite:- normal
•Sleep:- adequate 8 hrs per day
•Bowel and bladder :- regular
•Addictions:- ☆chronic alcoholic since 20years
-360 ml per day, stopped drinking since 1 month.
☆ Chronic smoker since 30 years - 2 packs per day .
•Occupational history:-hotel owner
GENERAL EXAMINATION:-
Patient is conscious, coherent and cooperative well oriented to time, place and person.
•Height:-158cm
•Abdominal girth: 124cm
VITALS:-
•Temp: afebrile
•Pulse rate: 90bpm
•Respiratory rate: 22
•BP: 130/80
•SpO2:98
Pallor, cyanosis, clubbing, are absent
Edema-pedal( pitting)
Icterus present .





SYSTEMIC EXAMINATION:-
●ABDOMINAL EXAMINATION:-
☆Inspection:
Abdominal distended
Umbilicus everted
Engorged veins present
No visible peristalsis
No scars , sinuses .
☆Palpitation:
Soft non-tender
no hepatomegaly or splenomegaly
☆Percussion : Shifting dullness
☆ Auscultation:- Bowel sounds heard.
● CVS :- s1,s2, heard , no murmurs present.
●RESPIRATORY SYSTEM:- Normal vesicular breath sounds heard.
● CNS:- No focal neurological deficit seen.







Ecg....

Chest xray

2D echo
.png)



PROVISIONAL DIAGNOSIS:-
Chronic liver disease with portal hypertension .
TREATMENT: -
1.Tab Lasix 80 mg po OD
2.Tab Aldactone 50mg BD
3.Tab Lactulose 20ml ODHS


Comments
Post a Comment